Category: Money | Reading time: approx. 10 minutes
Most psychiatrists thinking about private practice are asking the wrong question.
They ask “how much can I make?” when they should be asking two questions: how much do I actually need to make to live the life I want, and what kind of practice structure will get me there with the least friction?
Those questions matter more than the ceiling, because the ceiling is genuinely high — high enough that most psychiatrists significantly overestimate how hard they’ll have to work to reach a sustainable income. The numbers I’m going to walk through in this post would have sounded fantastical to me when I was still in academia. They are not fantastical. They are completely typical for psychiatrists running well-designed cash-pay practices today.
Let’s start with the assumptions that keep most people stuck.
The Income Myths Keeping You Stuck
Before we get to the actual numbers, I want to name the three beliefs I encounter most often when psychiatrists are thinking about leaving employed positions or insurance-based practice. These beliefs are not minor. They cost real money.
Myth #1: “My employed salary is the ceiling.”
This is the most expensive belief in medicine. Many academically employed psychiatrists earn between $220,000 and $280,000 per year working 40 to 50+ hours a week. They assume that’s roughly what a private practice psychiatrist makes — maybe a little more, maybe a little less, but in the same neighborhood.
That assumption is wrong by a significant margin. A well-designed cash-pay private practice can generate that same gross income in 20 to 25 hours a week of clinical time, which means a psychiatrist working a full week can earn substantially more. The math is not complicated. It’s just rarely shown to you.
Myth #2: “I need a perfect, fully built-out practice to make real money.”
You don’t. You need a minimum viable practice, a clear niche, and the willingness to charge what your time is actually worth. Some of the highest-earning private practice psychiatrists I work with have remarkably simple setups — a few well-chosen tools, a clean website, and a focused offer. Complexity is not what drives revenue.
Myth #3: “Charging cash means I’ll only serve wealthy patients.”
This is partially true and worth being honest about. Yes, cash-pay practices serve patients who can afford to pay out of pocket or who have strong out-of-network benefits. But many of those patients are not what you might assume — they are middle-class people who have prioritized mental health spending because the care they need is not adequately available through insurance. Many use HSA/FSA dollars or submit superbills for partial reimbursement. The patient demographic is broader than the stereotype.
I’ve written extensively about the ethics of cash-pay practice, including the video Is a Cash-Pay Psychiatry Practice Unethical? if this is a concern you’re still working through.
Cash-Pay vs. Insurance Math: The Side-by-Side
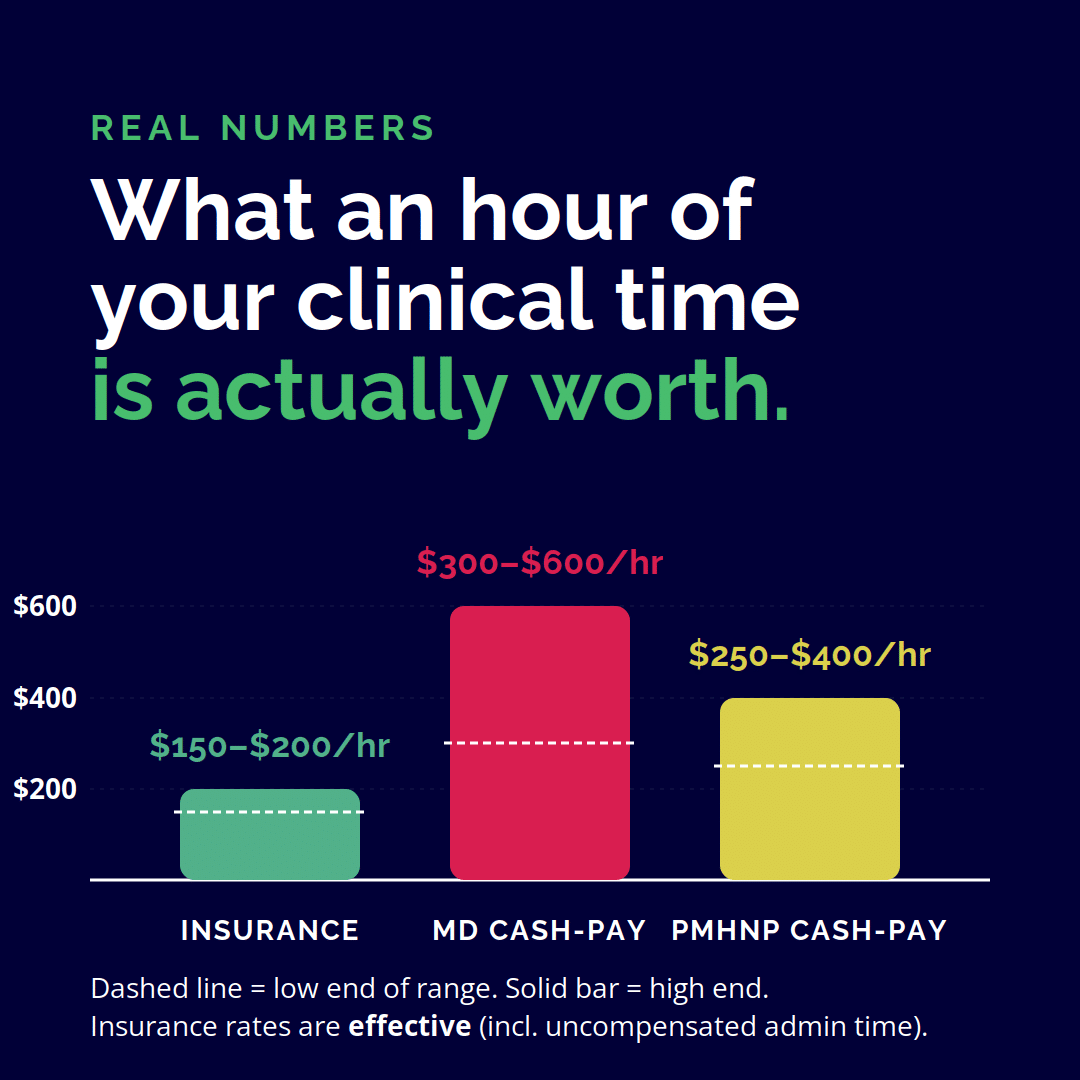
Let’s look at what an hour of your clinical time is actually worth in each model. These are real, current-market numbers — not theoretical maximums.
Insurance-based reimbursement
Most insurance panels reimburse a 99213 follow-up at $90–$130 and a 99215 at $140–$180. A new patient evaluation (90792) typically reimburses $200–$280. After insurance contract overhead, billing services, claim rejections, and unpaid prior authorization time, the effective hourly rate for most insurance-based psychiatrists comes out to roughly $150–$200 per hour of actual clinical work.
That is not bad. But it is also not the full picture, because that hourly rate does not include the 15–20 hours per week that most insurance-based providers spend on uncompensated administrative work. When you factor that in, the effective hourly rate drops meaningfully.
Cash-pay rates
Established cash-pay psychiatrists in most U.S. metro areas charge between $300 and $600 per hour of clinical time, with intake evaluations typically priced between $500 and $1,200. PMHNPs running well-positioned practices regularly charge $250–$400 per hour, with intakes between $350 and $1,000.
These are not aspirational numbers. They are current market rates. Alysha Woods, a PMHNP in my mentorship program, raised her intake fee from $350 to $1,000 over the course of the program. Jamie Gustafson, also a PMHNP, moved her rate from $125 to $300+ per hour after transitioning out of insurance. David Spielman, a psych NP specializing in ADHD and autism, went from $10K/month to $30K/month in five months by refining his niche and his pricing.
The hourly rate difference between insurance and cash-pay is significant. The bigger difference, though, is that the cash-pay hourly rate is what you actually take home for each hour worked — not a gross number eroded by uncompensated administrative time.
Revenue Scenarios: What Different Practice Sizes Actually Earn
The most useful way to think about private practice income is in scenarios, not single numbers. Different practitioners want different lives. Here are four realistic scenarios for a cash-pay psychiatrist or PMHNP, using conservative middle-market rates.
Scenario 1: The Part-Time Practice
10 clinical hours per week at an average rate of $400/hour, 48 working weeks per year. Gross revenue: roughly $192,000 annually for 10 hours of clinical work per week. This is a common starting point for psychiatrists keeping their employed position while building. After expenses (typically 15–25% of revenue for a lean practice), net income lands in the $145,000–$165,000 range.
Scenario 2: The Sustainable Full-Time Practice
20 clinical hours per week at an average rate of $400/hour, 48 working weeks per year. Gross revenue: roughly $384,000. Net income, after expenses, typically lands in the $290,000–$325,000 range. This is the bracket most psychiatrists in my program target — a practice that earns more than a typical academic salary while working roughly half the clinical hours.
Scenario 3: The Optimized Practice
25 clinical hours per week at a higher average rate of $500/hour (achievable with a strong niche, premium positioning, and 3–5 years of practice maturity), 48 weeks per year. Gross revenue: roughly $600,000. Net income typically lands in the $450,000–$510,000 range. This is the scenario most often associated with the publicly visible $30K/month figures — Kate Salama, Jess Romeo, David Spielman, and others in my program who are operating in this bracket.
Scenario 4: The Scaled Practice
Beyond the solo optimized practice, some practitioners scale by adding associate clinicians, group programs, courses, or supplemental products. This is where revenue can climb into the $750K–$1M+ range, though it represents a different kind of work — you become a business owner managing a practice rather than a clinician. Many psychiatrists are happiest stopping at Scenario 2 or 3. Not everyone wants to run a business beyond a sustainable solo practice. Both choices are valid.
The point of these scenarios is not to tell you which one to aim for. The point is to show you that the income range available in private practice is wide — and that the bottleneck is rarely demand or capability. It’s structure.

What Actually Comes Out of That Revenue (Real Expenses)
Gross revenue is exciting. Net income is what matters. Here is a realistic breakdown of what a solo cash-pay psychiatry practice actually spends, in approximate monthly costs for a mid-sized practice.
- EHR / practice management software: $50–$200/month (my favorite and recommendation is IntakeQ/PracticeQ)
- Telehealth platform (if separate): $0–$100/month — some EHRs include this
- Malpractice insurance: $100–$300/month for telepsychiatry practice
- Business banking + accounting software: $20–$80/month
- Website + domain: $20–$100/month
- Email marketing + scheduling tools: $50–$200/month
- Marketing spend (if any): $0–$1,000/month depending on strategy
- CME and continuing education: $100–$400/month averaged annually
- Bookkeeper or accountant: $200–$600/month
- State licenses, DEA, board certifications: $100–$200/month averaged
- Virtual assistant or part-time admin (optional): $500–$2,500/month
For most solo cash-pay practices without a virtual assistant, total monthly overhead runs $700–$1,500. With a virtual assistant or part-time admin, you’re typically looking at $1,500–$3,500/month. As a percentage of revenue, well-run solo practices keep expenses at 10–20% of gross.
The leanness of these numbers is one of the things that surprises new private practice owners the most. Compared to almost any other business model — a brick-and-mortar storefront, a tech startup, an agency — a telepsychiatry private practice has remarkably low overhead and remarkably high margins.
If you want to see exactly what these systems and tools look like in a working practice, How to Optimize & Scale Your Psychiatry Private Practice in 2024 walks through the operational backbone in detail.
Is There an Income Ceiling? (And Where It Actually Is)
There is a ceiling, but it’s probably not where you think it is.
In a solo cash-pay psychiatry practice, the practical ceiling for full-time clinical work — meaning 25 to 30 clinical hours per week at premium rates — is roughly $500K to $750K per year. This assumes a strong niche, established positioning, and the willingness to charge at the higher end of the market for your specialization.
Above that, growth tends to require structural changes: adding clinicians, building group programs, creating digital products, or developing a separate business line (training, supervision, courses). These can scale total revenue into seven figures, but they require building a business beyond your direct clinical work — a meaningfully different undertaking with its own complexity.
The honest answer to the income question is this: a well-structured solo cash-pay psychiatry practice can sustainably generate $300K–$500K in net income working roughly half the clinical hours of a typical academic appointment. That number is not aspirational. It is the median outcome for psychiatrists who execute the fundamentals well over 12 to 24 months.
The ceiling above that exists, but most psychiatrists hit a different ceiling first — the ceiling of “how much income do I actually want” versus how I want to spend my time. Many of the most thoughtful private practice psychiatrists I know have explicitly chosen Scenario 2 or 3 income levels in exchange for fewer clinical hours, more time with family, and meaningful work outside of patient care.
That is not settling. That is choosing.
So How Much Do You Actually Need to Make?
Here is the question I want you to sit with.
If you had a private practice that generated $300,000 in net income, with 20 clinical hours per week and the autonomy to design every other part of your life around your values — what would that change for you? Would it be enough? Would the answer be different from the income you have right now?
Most psychiatrists, when they actually do this math, find that the income they need is significantly lower than the income they’re currently structuring their life around to earn. Their employed salary is providing roughly the same net income as Scenario 2 — but it requires double the clinical hours, comes with administrative dysfunction, and offers a fraction of the autonomy.
The income question is not really an income question. It’s a structure question. Once you see that, the decision to build something different gets a lot clearer.

What to Do Next
If this post made you think “wait, those numbers are actually achievable for me?” — yes. They are.
Here are three actions, depending on where you are right now:
- If you’re trying to figure out your specific income target: Calculate your actual minimum viable income — the post-tax income you need to cover your real-life expenses plus savings goals. Then back into how many clinical hours per week at what rate would get you there. Most psychiatrists are shocked at how few hours that math actually requires.
- If you’re ready to understand the practice model that produces these numbers: Read How to Build a Cash-Pay Psychiatry Practice (linked below). It walks through the structural foundation.
- If you want a personalized look at what your specific income could look like: Schedule a free consultation call with my team. We will look at your situation — your state, your specialization, your financial goals — and tell you honestly what’s realistic and how to get there.
And if you want to see how the practice infrastructure that produces these numbers actually gets built, How to Build a Cash-Pay Psychiatry Practice is the most thorough starting point on this site.
The income is available. The infrastructure is teachable. The only thing left is the decision to build it.
Ready for your next step?
Want a clear, step-by-step plan for building your dream private practice (without the overwhelm)? Grab the free Private Practice Roadmap by answering a few quick questions below. It’ll help you get clarity on your next best steps, avoid common early mistakes, and start creating a practice that actually fits your life and values.
Leave a Reply